Feb 2, 2020 | Healthy Tips
WHAT IS CORONAVIRUS?
By: Colleen Doherty, MD
1/31/2020 UPDATE: The newest strain of coronavirus, called 2019-nCoV, surfaced in Wuhan, China, at the end of 2019. The Centers for Disease Control and Prevention (CDC) has confirmed six cases to date in the United States, but has only detected one instance of person-to-person spread in this country. Therefore, 2019-nCoV is not considered to be spreading among communities in the U.S. at this time. CDC monitoring is ongoing.
Coronavirus is a common family of viruses named for its appearance of having a crown (corona in Latin means “crown”). The crown is composed of a protein, called the spike protein, that sticks out from the virus’s surface.1
There are different types of coronaviruses, and while the majority typically cause mild cold symptoms (e.g., runny nose or sore throat), more dangerous types, like the coronaviruses that cause Middle East respiratory syndrome (MERS) or Severe Acute Respiratory Syndrome (SARS), may cause more severe disease, including pneumonia, and even death.
It is impossible to tell the difference between coronavirus infections and other illnesses based on symptoms alone. While doctors need to take a careful history and perform a physical exam, laboratory tests are needed to accurately diagnose coronavirus infections.
At this time, there are no medicines a person can take to prevent or treat the virus itself. Treatment for coronavirus infections is supportive, which means that the patient is supported while the infection runs its course and the body’s immune system clears the infection.
Types and Transmission:
Coronaviruses belong to the family Coronaviridae, and there are seven types that can infect humans.2
Types:
Four common types of human coronaviruses cause symptoms of the common cold.
These four coronaviruses—229E, NL63, OC43, HKU1—are often referred to as community-acquired coronaviruses because they are common and infect people all over the world.3
The other three coronaviruses are more worrisome because they have been linked to severe complications, like pneumonia and death.
These three coronaviruses include:
- 2019 novel coronavirus (2019-nCoV)
- Severe acute respiratory syndrome coronavirus (SARS-CoV)
- Middle East respiratory syndrome (MERS-CoV)
Transmission:
In the United States, the coronavirus most commonly infects people in the fall and winter.4
Ways in which the virus can spread from person to person include the following forms of contact:
- Droplets (after someone who has the virus coughs or sneezes)
- Touch (e.g., shaking hands with an infected person or touching an object that contains the virus and then touching your mouth, eyes, or nose prior to washing your hands)
- Feces (fecal-oral spread from infected patients; rare)
Symptoms:
The four community-acquired coronaviruses usually cause “cold” symptoms in the upper respiratory tract, such as:5
- Runny nose
- Cough
- Sore throat
- Fever
- Headache
- Malaise
Sometimes, the coronavirus can affect your respiratory system and complications, like pneumonia or bronchitis, may develop.
These complications are more common in babies and the elderly, as well as people with a suppressed immune system or an underlying heart or lung disease.
MERS-CoV and SARS-CoV:
These serious types of coronaviruses jumped from animals to humans, and are potentially life-threatening.2
According to the Centers for Disease Control and Prevention (CDC), MERS-CoV usually causes fever, cough, and trouble breathing, which often then leads to pneumonia. Thirty to 40 percent of people with MERS coronavirus have died.5
SARS-CoV causes a similar illness of fever, chills, body aches, and respiratory infection which can be fatal.
There are still cases of MERS, mostly in the Arabian peninsula. There have been no cases of SARS in the world since 2004.
2019 Novel Coronavirus (2019-nCoV):
At the end of 2019, a new coronavirus, called 2019-nCoV, surfaced in Wuhan, China. Similar to MERS and SARS, this coronavirus likely jumped from an animal (probably a bat, although scientists are not completely certain) to a human, perhaps via some other species. 6
It appears that the 2019-nCoV infection is causing a severe respiratory (lung) illness similar to SARS. Common initial symptoms of the infection include fever, cough, fatigue, and muscle aches.7 Available data suggests while the disease can be severe and even fatal, it may not have as high a mortality rate as MERS or SARS. The medical community is still trying to get accurate data early in this outbreak.
Diagnosis:
The diagnosis of a routine coronavirus infection (cold symptoms) involves a medical history, including travel history, and a physical examination. Most often, the patient will be diagnosed with a cold, and sent home.
If your symptoms are severe, your healthcare team may order tests to specifically check for the virus. This is done by taking a sample of your blood and/or a swab from your nose or throat.
With the new concern for 2019-nCoV infections, symptomatic patients and their doctors have to be careful to obtain a travel history to China or other infected regions, or a history of contacts with other people who may have been exposed. Laboratory testing for 2019-nCoV is currently being coordinated with public health offices and the CDC.
Treatment:
There is no vaccine or specific medicine to treat coronavirus. Instead, the treatment for mild coronavirus infections is supportive, which means doing things to ease your symptoms.8
These supportive measures may include:
- Taking a medication, like Tylenol (acetaminophen), to reduce your fever
- Using a cool-mist humidifier to help soothe your cough
- Rest
- Drinking fluids
Important Note:
Do not give your child or teenager aspirin or aspirin-containing products due to their risk of Reye syndrome, a potentially fatal condition.
SARS, MERS, and illnesses caused by 2019-nCoV also require supportive care, of a different type: hospitalization, oxygen, fluids, and other life-saving treatment may be necessary to support the patient while the immune system responds to, and clears, the infection.
Antiviral medicines shown to suppress or destroy coronaviruses are currently commercially available.
Prevention:
You can reduce your risk of contracting human coronavirus by doing what you would do to protect yourself from getting the flu or common cold:8
- Scrub your hands with soap and water for at least 20 seconds (try singing the Happy Birthday song twice for proper timing)
- Avoid touching your eyes, nose, and mouth
- Avoid being around people who are sick
If you are sick, you can protect others by staying home from work or school.
If you do cough or sneeze, be sure to cover your mouth and nose with a tissue, and then wash your hands after discarding the tissue. Alternatively, if you do not have a tissue available, sneeze or cough into the crook of your elbow.
A Word From Verywell:
Coronavirus is a common virus that infects people at least once over the course of their lifetime. The good news is that in most cases, it causes a mild, run-of-the-mill “cold.”
If your symptoms are severe or persistent, or if you have an underlying medical condition, be sure to see your doctor.
The 2019-nCoV coronavirus is concerning because of the potential for spreading globally, and because it can cause severe symptoms. As more information is gathered on this infection, we hope to remain a resource for you so you can get the information you need. If you are worried that you may have been exposed to this newly-described virus, it is a good idea to get medical care promptly.
Nov 13, 2019 | Healthy Tips
INTERMITTENT FASTING: THE DEFINITIVE GUIDE
By Alex Reed | Medically Reviewed By L.J. Amaral MS, RD, CSO
Intermittent fasting (IF) is one of the latest diet trends to hit the mainstream; however, this practice is really nothing new.
Humans have been fasting throughout most of history, mostly for religious but also for health reasons.
Science has only recently started to catch up with the health benefits of fasting.
So, you are saying that I should just fast and DHL will bring my six-pack and superpowers by tomorrow morning, right?
Well, probably not. There’s more than meets the eye when it comes to IF. That’s why, in this in-depth guide, I will teach you:
What IF really is and isn’t,
what happens to your body during it (the timeline)
and beginners guide to get started.
Let’s “fast” in.
What is Intermittent Fasting?
Intermittent fasting (IF), also called intermittent energy restriction, is an umbrella term for a range of dietary practices that involve defined periods of fasting and feeding.
The most basic definition of intermittent fasting is willingly abstaining from calories for a defined period of time. IF can be considered a variation of our normal eating patterns.(2)
Isn’t fasting the same as reducing calories?
Fasting can involve reducing calories, but it is not the same as controlled calorie restriction. There are no caloric guidelines for fasting.
Calorie restriction is achieved mainly by reducing portion size and limiting calorically dense foods.
Fasting, on the other hand, is done by controlling when you eat and not so much what you eat and how much you eat.
Why is IF So Popular?
Various forms of intermittent fasting had been practiced across the globe for ages, but only recently has it gained widespread attention. Why is this so?
“To eat when you are sick is to feed your illness.” – Hippocrates
Popularization in the media
Back in 2007, Brad Pilon, who is a fasting expert, published Eat Stop Eat, and many enthusiasts soon followed suit with their own material.
The biggest surge in popularity for IF happened around 2012 when BBC broadcast journalist Dr. Michael Mosley’s released his TV documentary Eat Fast, Live Longer as well as his book The Fast Diet.
Around the same time, author Kate Harrison’s published a book based on her own experiences titled The 5:2 Diet. The trend soon caught the attention of the scientific and medical communities (1), which labeled the growing trend as “the next big weight-loss fad.”
However, the popularity of IF only continued to grow, especially with the publication of Dr. Jason Fung’s 2016 bestseller The Obesity Code.
The “Blue Zones” book came out in 2008 showing the top 9 cities around the world that had on average the highest amount of centenarians. Valter Longo at USC has recently made headlines with his fasting-mimicking diet and how it reduces the burden of aging. (3)
Commercialization by companies
Another possible explanation why IF has hit the mainstream, particularly over the past two years, may have to do with its commercialization, at least according to Bloomberg (4).
You’d think that there’s no way you could sell products for a diet regimen that involves mimicking a state of fasting, or not eating (except water). However, we’ve witnessed products specifically targeted at those who fast regularly hit the dieting market, and these products include:
Diet plans and coaching
Electrolyte supplements
Appetite suppressants
Books
Weight-loss shakes
Full meal packages
IF apps
These companies have been heavily criticized for offering expensive products that are not backed by scientific evidence, especially in regard to IF.
Types of
Intermittent Fasting
There are many variations to intermittent fasting, with the most popular being time-restricted feeding (TRF) and whole-day fasting.
TRF involves eating only during certain times of the day and fasting for long stretches within one day. For example: One will fast until 12 PM and eat until 8 PM. This is called 16:8. Where for 16 hours you fast, and for 8 hours you eat.
Whole day fasting is going without food and caloric drink for 24-72 hours.
Both types can further be categorized into water fasts (with water) and dry fasts (without water) – the latter is not recommended since it will lead to dehydration and is usually only practiced for religious purposes.
TRF (time-restricted feeding)
The 16:8 fast – The most well-known IF method is the 16:8 fast. Originally popularized by Martin Berkhan of Leangains, the 16:8 fast is one of the easiest and most efficient fasting methods for weight loss. The numbers in the name stand for hours spent fasting and the hours of the feeding period (5,6).
The 20:4 fast – Also known as the warrior diet, the 20:4 fast was developed by Ori Hofmekler. On this diet, you fast for around 20 hours during which time you perform high-intensity workout and eat food within 4 hours. The feeding window may include two smaller meals or one large feast. This should not be done without proper medical supervision or proper planning and education as dehydration and hypoglycaemia (low blood sugars) can be deadly. (7)
OMAD – The One Meal a Day Diet (OMAD) involves fasting for 21-32 hours and eating for 1-2 hours each day. This method is great for fat loss but not so much for muscle building since the time for protein intake is very limited. (8, 9)
The 5:2 Diet – The fasting method popularized by Michael Mosley, the 5:2 diet involves eating normally for five days of the week with no restrictions, and then restricting calories to 500-600 per day for the other two days of the week. (10)
Fat fasting – As the name implies, fat fasting involves getting your calories only from fat for a period of time. This is to try and mimick your body’s state of fasting by going into ketosis. Bulletproof coffee is a popular drink taken during fat fasts. (11)
Dry fasting – Dry fasting involves total abstinence from all food and drink for a period of time, usually less than 24 hours. Fasting for Ramadan is the most well-known dry fast. (12).
Whole-day fasting
24-hour fast – Popularized by Brad Pilon, author of Eat Stop Eat, the 24-hour fast, as described in said book, consists of fasting for 24 hours twice a week and eating healthful foods for the other five days. (13)
36-hour fast – Fasting for one and a half day is difficult for most people, but it is definitely doable and safe when done correctly. In the past when food was scarce, not eating for this time frame was a normal occurrence. (14)
48-hour fast – Fasting for two days leads to major changes in metabolism and cell functioning. It can induce most people to go into ketosis, or fat-burning metabolism and lead to cell recycling and removing dead or damaged cells. (15)
ADF (alternate day fasting) – Fasting for one day and eating the next describes ADF. It is recommended to eat fewer calories on feeding days to promote weight loss. (16)
Extended fasting – Extended fasting is abstaining from food for up to three days. Little is known about the effects of prolonged fasting on humans, but animal studies found it can have profound effects on health. (17)
The Fasting Timeline
According to an article published recently in the journal Obesity, almost all fasting benefits are due to a “metabolic switch” that takes place 12-36 hours upon initiating fasting (18). But what exactly does this metabolic switch entail and when can one expect to gain fasting benefits? Chart source (*).
4-8 hours – After about 8 hours of fasting, which happens on a daily basis while you sleep for that long, the body has used up some of its glucose reserves (depending on your age, gender and body size) If you are on the leaner side, your body may go into “gluconeogenesis,” which simply means to make new glucose.
8-72 hours – Simultaneously, there is a dramatic drop in insulin levels, which soon signals fat cells to release fatty acids. Some of these fatty acids reach the liver to be converted into ketones (5). The longer you remain in a fasted state, the more ketones are being produced.
72 hours and onward – After 3 days of not eating any calories, the body enters “starvation mode” This means that metabolism is slowed down and the body will start breaking down its own fat cells for energy. If you don’t have a lot of fat reserves, the energy can come from breaking down muscle proteins. First, from dead intestinal cells and pancreas secretions and, later, from the muscle (1,20). Chart source (*).
Fasting for short periods of fasting intermittently triggers a host of adaptive responses that are good for health. These include things like increased cell renewal, activation of longevity genes, and increases in human growth hormone (21,22,23). However, fasting that becomes starvation can cause harm.
IF and Weight Loss
Most people nowadays are interested in intermittent fasting as a way to lose weight. And they’re not wrong for doing so. Studies found that both long-term and short-term fasts produce weight loss (24,25).
What’s really great is that compared to low-calorie diets, fasting does not lead to muscle wasting and leads to over 7 pounds more compared to low-calorie diets (26).
Researchers believe fasting produces weight loss mostly from fat burning through the following mechanisms (27):
It lowers insulin levels – Insulin is used to make cells grow. It is a key driver of weight gain by promoting fat storage and curbing fat burning in cells. Lower insulin during fasting happens as a result of drops in blood glucose, glycogen depletion, and weight loss. (28) Chart source (*).
It makes you eat less – Ideally, you should end up eating less within a 24-hour period when fasting is included. Fasting helps achieve lower calorie intake by limiting the amount of time you eat in a day. However, some people end up bingeing during their feeding windows, and this can prevent weight loss.(29)
It increases human growth hormone (HGH) – HGH is a hormone produced by the pituitary gland, a small gland in the brain. This hormone increases the breakdown of fat, counteracts the effects of insulin, and stimulates protein production (good news for muscle building). Fasting is able to increase this hormone significantly.(30) Chart source (*)
It kickstarts ketosis – Ketosis is often referred to as fat-burning mode. When you burn carbs for fuel, you produce glucose. When you burn fat for fuel, you produce ketones. During fasting, most ketones produced come from stored fat being used for energy. So, getting into ketosis regularly through fasts can boost your fat-burning potential. (31)
Fasting also improves insulin sensitivity and improves blood glucose levels – both important when it comes to weight maintenance. (32)
IF and Keto Diet
Intermittent fasting and the keto diet have one major thing in common – they can both get you into ketosis. Both dietary strategies induce this metabolic state, and for this and other reasons, many like to combine the keto diet with IF to improve their outcomes. In fact, Jason Fung, author of The Obesity Code, recommends the keto diet as a foundation for fasting.
When IF is practiced alongside a keto diet, it helps speed up transitioning into ketosis. That’s because going without food depletes liver glycogen sooner as does eating a diet low in carbohydrates, and this is an important precursor to ketosis. (31)
Some keto dieters also find that IF is much easier when practiced with a keto diet.
“The brain will rely less on glucose for energy when in a state of nutritional ketosis. Therefore, the transition into a fasted (ketogenic) state during the day eventually becomes seamless after eating low-carb or ketogenic for a few weeks (32).”
– Dominic D’Agostino, associate professor at the University of South Florida in Tampa and leading researcher in the field of Ketogenic diets and Cancer.
In other words, you won’t feel hungry, dizzy, and weak when fasting on a keto diet since your body is already adjusted to using fat for fuel and is relying less on glucose. This is because the state of ketosis mimicks the state of fasting in your body.
This is especially true if you’ve been on a keto diet for at least 4 weeks, which is the minimum time it takes to become keto-adapted – able to successfully use fat for fuel. (33)
However, if you’re not keto-adapted, IF may lead to worse keto flu and other adverse symptoms (34). On the bright side, combining the two may lead to greater weight loss since fasting makes you eat less during the day while keto supports fat burning.
Benefits
In case you need more convincing to try out IF, consider the following science-backed benefits linked to this dieting method:
“I fast for greater physical and mental efficiency.” – Plato
Weight loss – Low-calorie diets without exercise are not effective for weight loss because they reduce metabolic rate and lead to muscle wasting (35). IF, on the other hand, is great for weight loss because it leads to eating fewer calories, improved metabolic functioning, and enhanced fat burning, all the while sparing muscle tissue and maintain normal metabolic rate (36).
Longevity – Fasting boost autophagy, which is essentially your cells’ recycling system that helps eliminate dysfunctional cell components (37). With fewer damaged cell components, cells tend to function better and this can help you live longer.
Metabolic health – Fasting lowers blood glucose, insulin, and lipids while upregulating fat oxidation. This, in turn, leads to better metabolic health by increasing weight loss, insulin sensitivity, and the body’s ability to use energy efficiently. (31)
Inflammation – Fasting reduces inflammation according to studies done in rheumatoid arthritis (RA) patients (38). The anti-inflammatory benefits of fasting can also help with conditions like diabetes, obesity, and depression.
Hypertension – Studies also show that 13 days of water-only fasting leads to drops in systolic blood pressure (BP) below 120 in around 80% of people with borderline hypertension (38). However, we don’t recommend fasts this long without medical supervision.
Cancer – Researchers believe fasting may protect from cancer by reducing cell and DNA damage and by enhancing the death of pre-cancerous cells (38). It works against cancer through its effects on insulin, glucose, ketones, and specific hormones.
Convenience – IF allows you to think less about food by spending less time eating it. It’s also easy to follow and does not cost you money.
Side Effects
A systematic review involving 768 cases of patients water fasting mostly for 2 days found that most (65%) experienced only mild side effects and there are no reported deaths (39). The side effects these patients experience included:
- Fatigue
- Insomnia
- Headache
- Digestive issues
- Indigestion
- Back pain
- Hypertension
- Dizziness
Other common fasting side effects are unrelenting hunger, constipation, and irritability. Most of these side effects are due to dehydration, electrolyte changes, and low blood glucose levels (40). Some, like insomnia, are due to the stress of fasting and others, like stomach pain and indigestion, are due to high stomach acid levels.
More serious side effects of fasting like hair loss, water retention, menstrual irregularity, nutrient deficiencies, metabolic acidosis, and organ damage are reported in only extended fasts lasting several weeks (41).
Another serious side effect of extreme fasting and that you should be aware of is refeeding syndrome. It’s a result of a shift in fluids and electrolytes that happen when someone who is starved suddenly eats too much food. Luckily, this happens only with prolonged fasting of 10 days and more and rarely with normal IF (42).
IF is NOT for Everyone
Who should avoid IF
Wilhelmi de Toledo, a physician and fasting expert who is also the founder of the Medical Association for Fasting and Nutrition, made the first peer-reviewed fasting guidelines in English together with her colleagues (43).
The guidelines specify that people with the following should not fast:
- Recent unintentional weight loss and muscle wasting due to illness
- History of anorexia nervosa and other eating disorders or disordered eating
- Untreated hyperthyroidism
- Problems with blood supply to the brain and dementia
- Advanced liver or kidney diseases
- Pregnancy and nursing
Type 2 Diabetes on glucose lowering medications (without medical supervision)
Furthermore, the guidelines specify that those with the following should fast only under medical supervision:
- Type 1 diabetes
- Addictions
- Psychotic disorders
- Severe coronary artery disease
- Retinal detachment
- Peptic ulcers
- Cancer
Besides that, if you’re taking the following medication, your doctor may need to make dose adjustments when you fast:
- Non-steroidal anti-inflammatory drugs (NSAIDs)
- Systemic corticoids
- Antihypertensives (especially beta-blockers and diuretics)
- Glucose lowering medications for diabetes
- Contraceptives
- Anti-coagulants
- Psychotropics (especially neuroleptics and lithium)
-
It’s different for women
If you’re a relatively healthy woman who’s not pregnant or breastfeeding, you can definitely fast. However, if you’re underweight, pregnant, or breastfeeding, then this may not be a good time to fast.
Studies show that being underweight is just as bad for health as being overweight (44). Being underweight can also lead to fertility problems in women, especially when combined with fasting. Since fasting is known to lead to weight loss, it is not a good idea to do fasting when you are already underweight.
Fasting during pregnancy can starve both the mother and baby and increases a baby’s exposure to stress hormones according to one systematic review. Not to mention, you have higher protein and calorie needs while pregnant. This is not recommended. (45)
Fasting during breastfeeding may put a woman at risk of ketoacidosis (46). That’s because milk production is an energy-demanding process, and the body will break down fat stores at a fast rate to meet these energy demands. Breast-feeding burns about ~500 extra calories ahead, which you need to produce enough milk. Do not fast while breast-feeding. (47)
Who should try it?
If you’re relatively healthy but overweight, you can try IF to lose weight and improve other aspects of your health. You may want to start out with fasting for 12 hours first and then increasing your fasting time in a stepwise fashion.
If you’re a normal weight adult, you can use IF to boost longevity, your health, and your well-being. In this case, it is essential that you eat enough calories to sustain your current weight during your feeding window to prevent unnecessary weight loss and reap the benefits of fasting.
Besides weight loss, reasons to try fasting include improved ketosis, better metabolic health, lower risk of cancer, better brain functioning, and improved cardiovascular health. (3)
Can You Eat and Drink During IF?
Can you eat during IF?
IF is defined as someone willingly abstaining from food and drink during a specified time window that contain calories. Thus, drinks with no calories are allowed during the fasting window.
All food contains calories, so you cannot eat anything during your fasting windows. You can, however, consume non-nutritive supplements and liquids.
The only time you can and should eat during IF is within the defined feeding windows (like the 8-hour window during the 16:8 method) You can eat anything you want during this time but opting for nutrient-dense and healthful foods is recommended in order to get the most health benefits out of fasting
If your goal is weight loss, go for foods that help lower your calorie intake. Good examples are high-fiber vegetables, like cucumbers, celery, salads, broccoli, jicama, bell peppers, good fats like avocados, olives, nuts and protein-rich foods like eggs, fish and grass fed meats.
Can you drink during IF?
Dry fasts, like Ramadan, forbids drinking any fluids within the duration of the fast. All other fasting, on the other hand, involves adequate intake of zero-calorie fluids. These fluids include: plain water, fizzy mineral water, regular black coffee (sugar-free) and tea (sugar-free).
Juices, shakes, soups, and other calorie-containing liquids will break your fast. If you’re worried about electrolyte imbalances during fasting, consider zero-calorie electrolyte supplements or try drinking water with a bit of salt.
Adequate hydration during IF will make the fast safer and more tolerable. It will also keep your energy levels up. “Even mild dehydration can drain your energy and make you tired” according to the Mayo Clinic (48). You are already moderately dehydrated if you are thirsty. (49) The recommended daily fluid intake to prevent dehydration is:
15.5 cups (3.7 litres) for men
11.5 cups (2.7 litres) for women
The most common is to take your body weight in pounds and divide into 2 to get the amount of ounces you should be drinking per day. (50)
Can you take supplements during IF?
You can, but you don’t need to take supplements to get the fasting benefits.
There can be a time and place for them, and if done correctly, you can take supplements and fast successfully. In fact, there is one case reported in the medical literature where a man lost a significant amount of weight fasting while taking multivitamins (51).
Most multivitamins and other supplements contain a small number of calories, around 5 kcal per serving. Some contain sweeteners like fructose, and you may want avoid those. Make sure to read the label and know that the minuscule calories found in most supplements are unlikely to adversely affect your fast.
If your main fasting goal is ketosis, you may also use MCT supplements. The body prefers using medium-chain triglycerides (MCTs) for ketone production and they were found to promote weight loss (52).
How to Get Started
Most of us are fairly accustomed to eating every day, several times a day. As a result, this habit is hardwired in our brain, and the body will not be happy when you don’t give it its highly anticipated meal.
In fact, studies show it will respond with a surge in stress hormones when deprived (53). But the body can also adapt, especially if you prepare ahead. Here is how to do exactly that for easier fasting.
Start gently – If you’re not used to fasting, then go with a 12:12 fast first before experimenting with longer fasts. This fast is probably the easiest and safest to follow. It essentially involves having your last meal let’s say around 6 PM, and your next meal around 6AM. If you already do this, great! Go for 14:10, eating from 8 AM to 6 PM and continue to cut back on the hours eating during the day. This is the safest and easiest on the body.
Prepare ahead – Have a nourishing meal and plenty of rest the day before your fast. When we say nourishing, we mean a meal that contains adequate calories from fat, protein, and carbohydrates as well as fiber and micronutrients. A good example is a tuna and mayo salad with mixed greens, chicken breast over salad, or a hearty lentil and vegetable soup.
Drink plenty of water – Have a bottle of water with you at all times. Avoid diuretics like too much caffeine and alcohol. However, if you’re on a keto diet protocol, then a cup of Bulletproof coffee is perfectly acceptable and may help keep your energy levels up.
Stop if you’re unwell – A bit of hunger and fatigue are normal during your first fast. However, if you’re disoriented, unable to walk, feel shaky and dizzy, nauseated, have a headache or extremely irritable – it’s a good idea to break your fast.
Practice mindfulness – Not eating anything pretty much goes against our survival instincts, and this can easily put you in panic mode. Dr. de Toledo recommends meditation and relaxation techniques as this will be a mind over matter kind of situation (54).
Exercise with caution – Exercising will keep your cardiovascular system healthy during long fasts and help preserve muscle strength. It also helps bring enough oxygen to tissue, keeps you warm, enhances the flow of lymph, and boosts well-being. It is essential that you do this while hydrated and is best done in the morning to avoid having symptomatic low blood sugars during the day.
Break the fast – No matter if you’re following the 5:2 diet, the 16:8 fast, or whole-day water fast, you should break your fast with an easily digestible first meal followed by a meal of your choice later during your feeding window.
How to Break a Fast?
All fasts need a gentle end. As outlined in de Toledo’s fasting guideline, cooked or raw fruit and potato soup are typically served to break a long fast (55). Of course, if you’re on a keto diet, then bone broth or cauliflower soup or a fresh avocado and olives are better alternatives.
How gentle you should go depends on how long your fast lasted.
If you’ve fasted for two days straight, then go for vegetarian food like soups, olives, nuts and kefir are great options. Eat up to 800 calories during the first day of your fast break.
If you’ve fasted only for 8-16 hours, then break your fast with one vegetarian meal containing 300-400 calories and wait for a couple of hours before having your next meal.
Adequate fluid and fibre intake is also recommended to make the transition to eating safe and easy (56). This will also help with bowel movements.
The main reason why breaking fasts gently is recommended so that your digestive tract can slowly read just to having food intake again. Our bodies are used to eating food at the same time each day, and changes in our feeding schedule mean the body will have to adjust slowly to changes in feeding time.
Misconceptions
#1. Fasting is starvation
As Dr. Jason Fung puts in one of his blogs, the difference between fasting and starvation is a matter of willingness, i.e., if a person is willingly or unwillingly abstaining from food. (57).
Furthermore, fasting should entail “undernutrition without malnutrition” to yield benefits; otherwise, it can be labelled starvation (58).
#2. Isn’t it unhealthy to skip breakfast?
According to an opinion piece published in the 2014 issue of The Frontiers in Public Health, “breakfast is just another meal, …. prolongation of overnight fast, which depends not only on timing of breakfast but also on timing of the last meal of the day, can be beneficial (59).”
This piece as based on a literature review showing that there are no negative effects of skipping breakfast.
#3. Will fasting cause muscle loss?
Only if you don’t eat adequate calories and protein during fast breaks and are highly inactive.
Otherwise, evidence shows that fasting does not cause muscle wasting because it leads to ketosis, which is known to help preserve muscle mass and muscle functioning (60,61). This is especially true for overweight and normal weight individuals.
#4. Will fasting slow down my metabolism?
The rate of your metabolism, formally known as basal metabolic rate (BMR), slows down only during starvation.
Fasting, on the other hand, does not lead to drops in BMR, at least according to a study on 34 resistance-trained men who followed the 16:8 fast for 8 weeks (63).
#5. But aren’t we supposed to eat every 3 hours?
Eating small meals every couple of hours is said to help you eat less and burn more calories.
However, a study published in Obesity found that eating 6 small meals a day did not increase fat burning and may even increase hunger and desire to eat (64).
Eating fewer meals and keeping track of your daily calorie intake may be more effective.
#6. This is crazy, if I don’t eat for 24 hours, I’d die
As already explained, not eating makes your brain signal that you’re starving when you’re not. This leads to a surge in stress hormones like cortisol, which can further leave you feeling panicky.
Keep in mind that humans have been fasting since biblical times and that our bodies are perfectly designed to survive short periods of food restriction (24-48 hours). In fact, eating every few hours is new to the human race.
Besides, evidence shows humans can survive without food for up to 2 months (depending on fat stores) and without water only a couple of days (65).
Conclusion
Intermittent Fasting, an ancient practice and modern weight-loss trend, involves willingly abstaining from food and even drink for a short time frame.
The best way (for beginners) to fast intermittently is to start with 12 hour fasts, then 14 and get up to the 16:8 methods since it incorporates your overnight fast with your willing abstinence of only a couple of hours the following day.
Fasting this way provides a host of metabolic and adaptive benefits that are outlined in this article.
If you’re considering fasting for weight loss, metabolic health, cardiovascular health, or to manage a chronic disease, make sure to speak to your doctor first and do focus on fluids and being moderate with whichever method you choose.
https://bodyketosis.com/intermittent-fasting/
Sep 26, 2019 | Healthy Moves
BY: VICTOR OWENS
Everybody knows that physically active people have significantly better cardiovascular health. Every doctor in the world will advise you to get fit, feel better, and reduce your chances of joining the quarter of a million people in the United States who literally die every year simply from a lack of exercise.
Doctors used to believe that, while there was a great deal going on behind the scenes in cellular terms, the concept was really that simple. What has more recently been discovered is that prolonged inactivity has risks of its own – even for otherwise fit people. Even if someone performs high-intensity exercise several times a week, sitting for too long at a stretch can still put them at risk.
So, how much time do you spend on your rear every weekday?
When you actually add it all up, the answer may surprise you.
The Science of Sitting
Sometimes when studying a complex system like the human body, scientists can’t really start with a question like “What are all the factors that contribute to cardiovascular disease?”. This approach is just too wide and general. Instead, they might study the health and habits of similar people who differ in one respect, to see if they can find a correlation.
In this case, drivers and conductors on public transport – who respectively sit a lot at work and don’t – were polled, and it was discovered that, on average, drivers die sooner. Now, if they had compared sitting and non-sitting professionals with different socioeconomic backgrounds and types of work, like lawyers and lumberjacks, such a difference wouldn’t be all that surprising. In this case, however, they could only speculate on what in the world was causing this.
The interesting thing, which has since been confirmed by additional research, is that the cause of death in different cases wasn’t only from one single condition, but could be any of several. In fact, people who sit for 10 hours or more per day are 34% more likely to pass away in the hospital than are those who take the occasional stroll around.
Health Effects of Sitting Too Long
There is actually a huge difference in the effects of sitting down on a park bench just to eat a sandwich and spending whole shifts glued to your chair. Although more research needs to be done, how you sit may be just as important. Cultures that tend to squat or sit cross-legged are possibly not affected in the same way. The amount of time you get up between seated sessions and what you do when you get up also has an effect – longer and more active being better. However, even a minute or two of walking every hour can prevent a great deal of harm. Consider the following:
- During long periods of little movement, your metabolism slows. This can contribute to obesity, which is by itself a risk factor for several diseases.
- This means your heart slows down, while most people also breathe less easily when sitting. At the same time, the pressure on your thighs can reduce the ability of blood to flow freely, so that fewer nutrients are delivered and waste products take longer to be removed from your organs and cells.
- The above offers one possible explanation of why long-term sitters are more likely to develop dementia.
- Although the exact mechanism is unknown, there are also reports that too much sitting causes anxiety and other mental health issues, including loss of concentration.
- The same change in metabolic rate makes your cells use less energy and respond differently to insulin, which may later develop into Type 2 diabetes. One study found an increase in risk of 20% for every two hours spent watching television daily (unhealthy snacking may also have played a role here, not only sitting).
- As your circulation slows and your leg muscles do no work, more blood begins to pool in your legs, so getting varicose veins becomes much more likely. Something similar applies to the formation of blood clots, a condition some joker has labeled “e-thrombosis”.
- Finally, people who spend more time sitting show higher levels of inflammation in their tissues, which has been linked to several types of cancer, particularly in post-menopausal women.
The Importance of Posture
Virtually every mammal in the world has a spine much like ours, but arranged horizontally. Humans have a mostly vertical spinal cord, which works out pretty well for us but only as long as we pay attention to how we stand and, especially, how we sit.
As a kid, your mother might have yelled “Sit up straight!”, mostly for aesthetic reasons and because of the way hunched-over people are perceived socially. However, this issue goes much deeper; especially for older, less fit, or overweight people whose spines aren’t as well supported by their back muscles.
When your shoulders slump forward, as they tend to do when sitting at a desk, your breathing automatically becomes shallower, contributing to many of the problems already mentioned. Perhaps more importantly, your skeleton and especially your spine are literally the framework that prevents you from collapsing into a floor-dwelling sack of meat. Abusing them is bound to lead to problems – often permanent ones. As the following graph shows, this is a problem for very many people.
If you spend a lot of time in front of a computer, please make a point of ensuring that your feet are comfortably flat on the floor, your thighs and forearms are approximately horizontal, and, unless you’ve made a habit of maintaining good posture, your back is straight, upright, and supported by the backrest.
This may be difficult to achieve with your current furniture, so consider investing in a good ergonomic chair. This can literally keep you from developing conditions like sciatica and spinal arthritis. To a less serious degree, it will also save you unnecessary pain.
More On Posture
With 33 independently-moving vertebrae and 31 pairs of nerves, the spine is an amazingly complex organ, both mechanically and electrically. As the diagram above shows, the nerves radiate out to regulate not only the movements of our limbs but also much of the function of our organs.
For this reason, one of the principles of chiropractic is that a spinal problem can manifest as any of a range of otherwise baffling medical problems. While many in the medical community continue to view chiropractors as little better than faith healers, anyone who has suffered a pinched nerve will know how uncomfortable this can be. Avoiding back pain, which often requires chronic medication, braces, or special sleeping arrangements, is therefore not the only reason to ensure that you sit up straight or at least stand up periodically.
Working Out In the Office?
One of the main reasons people spend too-long stretches glued to their chairs is that most offices and other workplaces are (nominally) designed and managed for efficiency, not workers’ health. This issue is no longer being ignored by employers, however. When taking into account the lost productivity and direct medical expenses of sick days and long-term absences, most are quite willing to consider implementing initiatives to keep employees healthy.
It’s clearly just a bad idea to force employees to suffer in unhealthy environments. Some companies are now providing on-site workout facilities with treadmills and showers, or at least subsidized memberships to nearby gyms. Others are realizing that ideas dating from the 1800s on how people should behave in the workplace are no longer relevant. In fact, allowing people to leave their desks and walk around every 30 minutes or so doesn’t turn them into hardened procrastinators; these planned interruptions actually make people more productive at their jobs, not less. This is called the Pomodoro method.
Numerous phone and computer apps make this technique easy to practice, while fitness bands like the FitBit actually start vibrating when you’ve been sitting down for an extended period. At this time, you could stretch, walk around, or perhaps get a glass of water. If you prefer, there are even exercises you can do, without leaving your chair, that will undo some of the damage caused by sitting motionless.
Using a Standing Desk
One of the most innovative and effective solutions to the entire problem is to use a standing desk. This does take some getting used to, especially for older people, but the reduced risk of lower back pain, heart disease, and diabetes makes it worth it. Your body is designed to work best when it’s either vertical or lying down, and all that’s needed to overcome the initial discomfort is practice. There is a caveat to this, though – if you’re currently sitting down for all or most of your workday, don’t try to make the change all at once, as your joints and muscles will do much better by dealing with a gradual transition. If possible, try getting a sit/stand desk that can switch between high and low positions.
One objection many people raise to working standing up is that standing will be too distracting to get much done. Actually, the opposite is the case. Have you ever attended a meeting where chairs were banned? These tend to be much briefer and productive, and not only because people’s feet start to hurt.
When you’re erect (and in the correct position), your breathing and circulation are much better. Considering that your brain uses about a third of the oxygen you inhale, this means that you’ll be more alert, able to concentrate and remember better.
Repairing the Damage
If you’re middle-aged or approaching it, you may already have noticed some signs that you’ve been sitting too much over the years. You might be a little heavier around the waist, get dizzy spells when you stand up too quickly, have high insulin resistance, or perhaps even have to carry a heart rate monitor band around with you.
The bad news is that there is simply no pill or surgery that will magically restore your body to tip-top condition. The good news is that relatively simple lifestyle changes – which you might want to make anyway – can have major effects.
The first thing to do is to start moving throughout the day. You don’t need to take up weightlifting or running – some doctors are now suggesting that frequent, gentle activity may actually be better for you than shorter bursts of exercise.
If you haven’t already, quit smoking and moderate your alcohol intake. Eat less sugar and saturated fat, but more vegetables and fruits.
All of these are things we know we should be doing anyway; they not only ameliorate the direct effects of years spent chained to the desk, but they prevent other problems too. Above all, don’t panic about your health. Go for checkups when needed and get a blood pressure monitor if you have to, but remember that stressing about these things will only make them worse.
THE HEALTH RISKS OF PROLONGED SITTING.
Sep 26, 2019 | Healthy Tips
By AMERICAN HEART ASSOCIATION NEWS
Scientists say there are indications of a potentially dangerous link between high rates of malaria and high blood pressure, and they are urging more research in hopes of better addressing harmful effects of hypertension in malaria –stricken areas.
A paper by researchers in Africa and the United Kingdom said there is reason to believe malaria and high rates of high blood pressure are linked in low- to medium-income countries — even among children.
That’s especially true in sub-Saharan Africa, where the infectious disease is so common and blood pressure levels are often high, the researchers wrote in the paper released Thursday in Circulation Research.
The paper’s lead author Anthony O. Etyang, M.D., a consultant physician and clinical scientist at the KEMRI-Wellcome Trust Research Programme, in Kilifi, Kenya, Africa, said the association makes sense for several reasons.
One is blood pressure tends to be high in parts of the world where malaria, a mosquito-borne infectious disease, causes flu-like symptoms, is prevalent.
Malaria can be deadly for those who aren’t treated. According to the Centers for Disease Control and Prevention, in 2015, there were an estimated 214 million malaria cases worldwide and 438,000 people died. Most of the dead were children in Africa.
Etyang said a second reason to believe there is an association is that malaria in pregnancy causes low birth weight, which has been shown in studies to be associated with the development of high blood pressure later in life.
Research published in Hypertension in January 2014 suggests that, in Nigeria, children born of mothers who suffered malaria tend to have higher blood pressures at 1 year of age.
“Because blood pressure patterns tend to be sustained over the course of time, these children are more likely to become hypertensive as adults,” Etyang said.
Yet another reason for the potential association, he said, is that malaria in childhood causes malnutrition and, especially, stunting.
“Malnutrition and stunting in childhood have also been shown in developed countries to predispose individuals to developing hypertension,” Etyang said.
In addition, he said, malaria in childhood causes inflammation, which, in turn, can lead to arterial stiffness and high blood pressure.
To test the hypothesis, convince others and encourage more research, the study authors reviewed scientific studies on high blood pressure and checked those that might also be associated with malaria.
They came up with different types of research that could reveal whether there is an association, including ecological studies, in which researchers would look at the distribution of a disease on a map and overlay it against the distribution of another disease or exposure to see if the two could be related.
They could do cohort studies; in which they would follow up with people for a long time to see if the subjects developed a particular disease. And they suggest Mendelian randomization studies, which use the backdrop of genetics to determine the contribution of environmental factors to disease development.
“If this link exists then it would be a game-changer in understanding malaria and hypertension. It might be possible to develop drugs that target the pathways activated by malaria that lead to hypertension. These drugs would be of great use in sub-Saharan Africa,” Etyang said.
It’s possible that if malaria causes high blood pressure, many other infectious diseases also could lead to hypertension, according to Etyang.
“Further research would be needed to see if factors arising during infectious episodes that lead to hypertension could be identified and treated along with the infection to prevent future adverse consequences,” he said. “Also, if this link exists, it would increase the economic benefit of eliminating malaria.”
High cardiovascular disease rates are indeed an area that needs more attention in low- and middle-income countries, and high blood pressure could be a main contributor to cardiovascular disease risk, according to Roger Bedimo, M.D., chief of the infectious diseases section at VA North Texas Health Care System and associate professor of medicine at UT Southwestern Medical Center.
But, Bedimo, who wasn’t among the researchers on the new paper, said he isn’t as confident there is a link between malaria and hypertension.
While it’s possible that malaria-induced low-birth weight will later lead to hypertension in adulthood, malnutrition from malaria infestation would predispose to hypertension later in life, and malaria-induced chronic inflammation would be a risk factor for cardiovascular disease, Bedimo said that he believes there are other, potentially better, explanations for high rates of hypertension in low- and middle-income countries.
“Behavioral factors such as salt consumption, which is rather liberal in many [low- and middle-income countries], would be a far more proximate cause of hypertension,” Bedimo said. “Should malaria indeed be associated with hypertension, there could be a rather more direct explanation that would need to be explored first, [such as] anaemia.
“Anaemia is a very frequent complication of malaria in endemic areas. Chronic anemia is, itself, a proven risk factor for enlarged heart and could well more directly predispose to hypertension,” he said.
SCIENTISTS PROPOSE A MALARIA-HIGH BLOOD PRESSURE LINK
Jun 28, 2019 | News
DIABETES
By: Michelle Llamas
Diabetes is a disease where blood sugar levels are too high because the body can no longer make or use insulin properly. The condition could lead to serious complications and even death. An estimated 29.1 million Americans have diabetes, according to the Centers for Disease Control and Prevention.
Diabetes in the U.S.
There are several types of diabetes, including Type 1, Type 2 and gestational — a type that occurs in pregnant women. All forms of diabetes involve high blood sugar levels. Type 1, an autoimmune disorder, is rare compared to Type 2. Type 2 is the most common, and about 95 percent of all people with diabetes in the U.S. have this type. An additional 86 million adults in the United States have prediabetes, a condition where your blood sugar is high but not elevated enough for a diabetes diagnosis.
Cases of diabetes increase each year, and every 19 seconds doctors diagnose someone in the U.S. with the disease. The Centers for Disease Control and Prevention (CDC) estimates that 1 in 3 adults may be diagnosed with diabetes by 2050.
It’s important to keep blood sugar levels controlled because it can cause serious health problems — including kidney disease, heart problems, skin problems and limb amputations.
FACT
Even if Type 2 diabetes has no cure, it can be prevented and managed. People with the disease can control blood sugar with lifestyle changes and medication.
Type 1 vs. Type 2 Diabetes
Type 1 diabetes is when the body simply does not make insulin. This type makes up about 5 percent of individuals living with diabetes. Type 2 diabetes is generally the result of a person’s body not producing or using insulin as efficiently as it once did (known as insulin resistance). Type 1 was previously known as “juvenile” diabetes. This is because Type 1 is most often diagnosed in children and young adults, although it can appear at any age.
What is Type 1 Diabetes?
Type 1 diabetes occurs when the immune system mistakenly attacks and destroys healthy tissue. An illness, such as an infection or virus like mumps, measles, rubella or the flu, or another trigger, can cause the body to turn on itself, mistakenly attacking cells in the pancreas that make insulin.
Type 1 is a life-long disease with no cure and no chance of remission. Treatment involves daily insulin injections. The exact cause of Type 1 diabetes is unknown.
What is Type 2 Diabetes?
Type 2 diabetes is a disease in which your body loses its ability to produce and use insulin, a hormone made by the pancreas that the body uses to convert glucose into energy. Without the right amount of insulin, excess sugar builds up in the body and causes a number of health problems.
EXPAND
Where Type 1 typically occurs in younger people and is an immune disorder, Type 2 most often occurs later in life. In fact, the medical community used to call Type 2 diabetes “adult-onset” diabetes. Most people with Type 2 are 60 and older, but doctors are diagnosing younger people with the disease. About 3.7 percent of adults aged 20 to 40 have the disease.
Type 2 diabetes is a progressive disease. This means that it may worsen over time and require higher doses of medication or multiple medications to control blood sugar. The pancreas may stop producing insulin altogether, and this means a person with Type 2 will need to inject insulin along with other medications.
An Estimated 29.1 million Americans have diabetes
About 95% Of all people with Diabetes have Type 2
An Additional 86 million Adults have prediabetes
History of Diabetes
Dr. Elliot Joslin publishes The Treatment of Diabetes Mellitus
Drs. Frederick Banting, Charles Best, then Banting’s assistant, and Professor J.J.R. Macleod extract insulin from dogs and discover it lowers blood sugar in dogs without a pancreas.
James Collip purifies insulin for use in humans. Banting and Macleod win the 1923 Nobel Prize in Physiology or Medicine for their discovery.
Elli Lilly and Company is the first company to commercially produce insulin.
The American Diabetes Association funds its first research grants.
Urine glucose testing tablets become widely available.
Oral medications called sulfonylureas that stimulate the pancreas to produce more insulin hit the market.
Drs. Solomon Berson and Rosalyn Yalow discover a way to measure insulin in the blood and identify “insulin-dependent” (Type 1) and “non-insulin-dependent” (Type 2) diabetes.
The first color-coded glucose test strips hit the market.
The first glucose meter becomes available.
Researchers discover insulin receptors, and defective receptors are linked to possible insulin resistance in Type 2 diabetes.
Link between hyperglycaemia and blood vessel disease discovered.
First insulin pumps invented.
Researchers use E. coli to produce insulin identical to human insulin.
Diabetes is classified into Type 1, Type 2, gestational and diabetes associated with other conditions.
FDA approved human insulin made by genetically altered bacteria.
Metformin becomes available in the U.S.
The drug Precose hit the market. Eli Lilly introduces the fast-acting insulin, Lispro.
Rezulin (troglitazone), the first of the thiazolidinedione class of diabetes drugs, hit the market. It was later removed from the market because of liver toxicity. Actos (pioglitazone), a drug in the same class, is available on the U.S. market, and some studies link it to bladder cancer.
Prandin (repaglinide) a drug in the meglitinide class, hits the market.
The American Diabetes Association defines prediabetes.
Byetta (exenatide) is the first incretin mimetic GLP-1 drug on the market.
FDA approves Januvia (sitagliptin), the first DPP-4 inhibitor.
Invokana (canagliflozin), the first SGLT2 inhibitor is available in the U.S.
FDA approves first automated insulin-delivery device (artificial or bionic pancreas) for patients 14 and older with Type 1 diabetes – Medtronic’s MiniMed 670G hybrid closed-looped system.
Diabetes Symptoms
Type 1 and Type 2 diabetes share similar symptoms. But Type 1 patients tend to experience symptoms sooner than Type 2 patients. This is largely due to that fact that the pancreas of a Type 1 patient does not produce insulin at all. Therefore, individuals with this form of the disease are affected much sooner and more intensely than those with Type 2. Type 2 patients actually make greater amounts of insulin for some time as insulin resistance builds. Eventually the body cannot keep up with the increased demand, insulin production begins to decline and Type 2 diabetes results.
Typically, in patients with Type 1 diabetes, their symptoms result in a diagnosis, whereas those with Type 2 may not even have symptoms or be aware of a problem until they are diagnosed.
Common Symptoms of Diabetes Include:
- Frequent Urination
- Feeling very hungry or thirsty
- Extreme fatigue
- Blurry Vision
- Bruises or wounds that are slow to heal
- Tingling, pain or numbness in feet or hands
- Dry itchy skin
LOW BLOOD SUGAR AND TYPE 1 DIABETES
Patients with Type 1 diabetes are more likely to experience symptoms of hypoglycaemia, or low blood sugar, than people with Type 2. This dangerous drop in blood sugar levels is usually due to patients with Type 1 taking more insulin than needed. Exercise, although still considered a lifestyle choice, can cause low blood sugar levels in people with Type 1 diabetes.
A drop in blood sugar can happen quickly in patients with Type 1 using insulin. Symptoms of hypoglycaemia usually appear when a person’s blood-sugar level falls below 70 milligrams per decilitre (mg/dL). These symptoms include headaches, hunger, nervousness, irritability, rapid heartbeat (palpitations), shaking, sweating, weakness, tiredness and nausea.
Risk Factors of Type 1 Diabetes
Although the cause of Type 1 is unknown, there may be a hereditary component. The tendency to develop autoimmune disorders, such as Type 1 diabetes, is typically passed down from one family member to the next, meaning some people may simply be more genetically prone to acquiring the disease. This seems to especially be the case for children born to fathers with Type 1 diabetes, according to one large family study of diabetes.
A certain genetic marker that has been shown to make a person more susceptible to Type 1 is located on a specific chromosome known as chromosome 6. A chromosome is a threadlike structure contained in the nucleus – the central part of a cell – where genetic information is held in the form of genes. The genetic connection for Type 1 is situated on chromosome 6 in the form of a human leukocyte antigen (HLA), which is a gene complex that encodes (produces) certain proteins responsible for the regulation of a person’s immune system.
However, having one or more of these HLA complexes does not always lead to the development of Type 1 diabetes. A genetic predisposition to Type 1 is just one factor among other possible risk factors making it more likely a person will develop the disease.
Other risk factors include:
Certain viral infections
Specifically, measles and mumps, among others
Race/ethnicity
In the U.S., Caucasians seem to be more susceptible to Type 1 than African-Americans and Hispanic-Americans, while people of Chinese and South American descent seem to have a lower risk of developing Type 1 overall.
Where a person lives
Northern climates seem to be at a higher risk for developing Type 1, especially in the winter months compared with a declining rate of diagnoses in the summer months.
Cow’s milk given at an early age
Children who are introduced to cow’s milk very young tend to have a slightly higher risk for developing Type 1 diabetes.
Other autoimmune conditions
Having an autoimmune disorder that shares a similar HLA complex to Type 1, such as Graves’ disease or multiple sclerosis (MS), can make a person more susceptible to Type 1 diabetes as well.
A less common cause of Type 1 diabetes is injury to the pancreas. This injury and damage to the organ and its cells can result from toxins, trauma or surgery.
Risk Factors of Type 2 Diabetes
Most people may be aware that being overweight increases the risk of developing Type 2 diabetes, but there are a few other factors. In fact, not all people with Type 2 are overweight. Diabetes is complex and no two people with the disease are the same.
The National Institute of Diabetes and Digestive and Kidney Diseases offers a checklist for Type 2 diabetes risk factors, it includes:
- Age 45 years or older
- Being overweight
- Parent, brother or sister with diabetes
- Family background: African American, Hispanic/Latino, American Indian, Asian American or Pacific Islander
- Gestational diabetes while pregnant or had a baby weighing 9 pounds or more
- Higher than normal blood glucose
- Blood pressure above 140/90 or “high normal” blood pressure
- High cholesterol levels, HDL lower than 35 or triglycerides above 250
- Being physically active less than three times a week
- Having discoloured, dirty looking skin in the armpits or around the neck despite scrubbing
- Blood vessel problems in the heart, brain or legs
Lowering Your Type 1 Diabetes Risk
A person’s risk for developing Type 1 diabetes often cannot be lowered or prevented since the disease is the result of an immune response. Several risk factors associated with the disease are also unable to be changed, such as one’s family history, genetic makeup, race or ethnicity, or other autoimmune conditions.
It may be possible, however, to prevent injury or damage to the pancreas that can sometimes result in the development of Type 1 diabetes. The pancreas can be easily injured due to its lack of protection from the ribcage. Pancreatic trauma, the term for injury to the pancreas, is most often caused by a car accident or a direct blow to the abdomen. The trauma that occurs can be the result of blunt force or penetration.
If a pancreatic injury is suspected, it is important to seek immediate medical attention, especially where there is blood loss, persistent abdominal pain or other symptom. Those conditions might include, inflammation, bruising, dizziness, nausea and vomiting.
Signs and symptoms of a pancreatic trauma can surface hours or even days after the injury occurs. Surgery is often necessary to treat an injury to the pancreas that results in symptoms. Pancreatic injuries can sometimes become life-threatening.
PREVENTING ACUTE PANCREATITIS
Acute pancreatitis is the sudden swelling and inflammation of the pancreas caused by enzymes in the organ eating and digesting its own tissue. This results in swelling, bleeding and eventual damage to the pancreas. Certain diseases, surgeries and habits, such as alcoholism or alcohol abuse, make a person more likely to develop the serious condition that results in severe injury to the pancreas.
Other factors linked to the development of acute pancreatitis include:
- Autoimmune problems
- Blockages in the pancreatic duct or common bile duct (tubes that lead enzymes from the pancreas)
- Damage to the ducts or pancreas caused during surgery
- High blood levels of a certain fat called triglycerides
Avoiding alcoholic drinks, smoking and fatty foods, and talking to your doctor about the risks of taking certain medications, can help to avoid pancreatitis or keep it from recurring after an attack.
Lowering Your Type 2 Diabetes Risk
The most effective ways to lower your risk of Type 2 diabetes are by making smarter food choices and increasing your physical activity. Experts recommend at least 30 minutes of activity each day. Of course, it is not always easy to make these changes overnight. The American Diabetes Association recommends making these changes over time so you can adopt them as a lifestyle.
Here are some tips for making small, sustainable changes:
- Set realistic goals and start slow.
- Set a timeframe to complete them.
- Keep goals specific.
- Reward yourself for accomplishing goals.
One misconception about lowering your risk by losing weight is that weight loss has to be significant, such as 50 to 100 pounds. The truth is losing as little as 10 pounds can have a dramatic impact on health and diabetes risk.
Diagnosing Diabetes
Symptoms of Type 1 diabetes generally develop early in life, when people are in their teens or when they are young adults. Type 2 symptoms generally develop later in life.
However, because the symptoms of Type 2 diabetes seem mild or might not appear at all, many people don’t know they have it. The American Diabetes Association estimates that 8.1 million people may be living with undiagnosed Type 2 diabetes. Many health care professionals can check for diabetes with simple blood tests.
There are three main tests for diagnosing diabetes, both Type 1 and Type 2, and prediabetes: fasting plasma glucose (FPG), A1C and oral glucose tolerance test (OGTT).
Fasting Plasma Glucose FPG (FPG)
This test measures levels of fasting blood sugar. Patients should be fasting for at least 8 hours prior to the test. This is the most popular test.
A1C
This test measures average blood glucose over the course of 2 to 3 months. It is a simple blood test and, like the FPG, patients must be fasting. Doctors may opt to do both FPG and A1C tests at the same time.
Oral Glucose Tolerance Test (OGTT)
Patients must be fasting with the OGTT. OGTT can also diagnose gestational diabetes. The patient’s blood glucose is measured before and after drinking a special sugary drink.
Ketone Testing
Ketone testing is another diagnostic method sometimes used to diagnose diabetes. This test is performed using a sample of the patient’s blood or urine. Ketone testing is generally used in diagnosing Type 1 rather than Type 2 diabetes because ketones in the urine are more commonly seen in patients with Type 1.
Ketones are chemicals produced when the body burns or breaks down fat for energy, or fuel. When the body lacks enough insulin to convert sugar, or glucose, to energy, it must break down fat instead. During this process, ketones form in the blood and infiltrate the urine, often making the patient sick.
Ketones in the urine, therefore, are a sign that the body is using fat instead of glucose for energy, thereby signalling that there’s not enough insulin and that as a result, a patient’s blood glucose level is likely too high.
Ketone testing can be done when the following conditions are present:
- When the blood sugar is higher than 240 mg/dL
- During an illness such as pneumonia, heart attack or stroke
- When nausea and vomiting occur
- During pregnancy
After Diabetes Diagnosis
A diagnosis of diabetes is serious, but with the right help people can take the correct steps to maintain their health. A diagnosis may mean many changes in lifestyle, but it doesn’t mean life is over. For example, the American Diabetes Association has a number of great resources to help make sensible lifestyle changes.
Many people may feel it is their fault they got Type 2 diabetes. But, this isn’t true.
What is true is that they must be more vigilant about their health. To that end, it is important to find the right professionals to help you manage your blood sugar. This may include your doctor, nurse, pharmacist, dietitian and diabetes educator. The diabetes care team can help create a treatment plan that works.
Diabetes Treatments
When doctors first discovered diabetes in the early 1900s, there were few options for treatment. It wasn’t until the 1990s that people with Type 2 diabetes had oral medications like metformin— still a mainstay of treatment for many people with diabetes.
Insulin, a necessary treatment for patients with Type 1 diabetes, remains one of the biggest medical discoveries to this day. Prior to its unearthing in the early 1920s, led primarily by Dr. Frederick Banting of Toronto, Canada, diabetes was a dreaded disease that led to certain death. A strict diet to minimize sugar intake, which sometimes caused death by starvation, was the most effective treatment, possibly buying patients a few more years to live.
Banting and one of his colleagues were awarded the Nobel Peace Prize for their discovery in 1923. That same year, drug manufacturer Eli Lilly started large-scale production of insulin, producing enough to supply all of North America.
Now, in addition to injected insulin, there are a number of oral medication classes to choose from, all with their own benefits and risks. But diet and exercise are still an important part of both Type 1 and Type 2 diabetes treatment. Now, even special types of surgery can help people with both types of diabetes manage their blood sugar.
A doctor may recommend one type of treatment or a combination of the three.
Medications
When changes in diet and increased physical activity are not enough to control blood glucose levels, doctors will prescribe medications. These same medications, aside from insulin, are not used, however, to treat patients with Type 1 diabetes. Insulin is the only medication prescribed to treat Type 1 diabetes, and Type 1 patients are required to take the hormone replacement daily. However, there are several different types, or classes, of medications available to treat Type 2 diabetes. Each controls blood sugar in different ways. Some people may take more than one medication to more effectively control sugar levels.
Type 2 Diabetes Groups
- Increase release of glucose through urination
- Increase insulin sensitivity of liver, fat and muscle cells
- Stimulate insulin production by the pancreas
- Slow the digestion of carbohydrates
There are many medications to treat Type 2 diabetes, and typically they are organized into groups that represent the condition that they target. These drugs are then organized into classes by mechanism of action.
SGLT2 INHIBITORS
A new class of diabetes medications called sodium-glucose co-transporter 2 (SGLT2) inhibitors release excess glucose in the body through urination. The FDA approved Invokana (canagliflozin), the first drug in the class, in 2013. Several others followed. But the agency has also released a number of warnings for serious side effects linked to these medications.
Popular Drugs in This Class Include:
- Invokana (canagliflozin)
- Invokamet (canagliflozin and metformin)
- Invokamet XR (canagliflozin and metformin extended release)
- Farxiga (dapagliflozin)
- Xigduo (dapagliflozin and metformin)
- Jardiance (empagliflozin)
- Glyxambi (empagliflozin and linagliptin)
Side Effects of SGLT2 Inhibitors May Include:
- Urinary tract infections
- Yeast infections
- Increased urination
- Diabetic ketoacidosis (DKA)
- Low blood pressure
- Increased cholesterol
- Hypoglycemia (low blood sugar)
- Nausea
- Fatigue
- Dry mouth
The FDA warned UTIs caused by SGLT2s can lead to other serious infections. The first is urosepsis, a serious systemic blood infection that can be fatal. The second is pyelonephritis, a serious kidney infection. Pyelonephritis may also lead to a blood infection. Both types of infection require hospitalization and antibiotics.
Additional FDA safety communications warned about kidney injury and diabetic ketoacidosis, a condition that occurs when too many toxins build up in the blood. New studies also show these drugs may also cause acute pancreatitis, a condition caused by the swelling and inflammation of the pancreas — the organ that produces insulin.
BIGUANIDES
Biguanides are a class of drugs that work by making the body more sensitive to insulin. They also stop the liver from making glucose and releasing it into the blood. They may also make fat and muscle cells more insulin sensitive.
Currently, there is only one drug in this class available on the market: Glucophage (metformin). This is one of the most widely used Type 2 diabetes medications in the world. Since it has been around since the 1920s, its side effects are very well known. It became available in the U.S. in the 1990s. Many doctors are very comfortable prescribing it as a frontline medication or in combination with other medications.
In fact, most combination oral medications contain metformin. Newer drugs also test their effectiveness against metformin in clinical trials.
Metformin’s Side Effects May Include:
- Nausea
- Decreased absorption of B12
- Skin rashes
- Lactic acidosis (too much lactic acid in the blood)
- Diarrhea
- Abdominal pain
THIAZOLIDINEDIONES (TZDS)
TZDs work by decreasing blood glucose levels by making muscle, fat and liver cells more sensitive to insulin. The FDA approved many of these drugs in the 1990s. The two most popular drugs in this class are Actos and Avandia. But these drugs were linked to serious side effects including bladder cancer and heart failure.
ACTOS (PIOGLITAZONE):
It has been one of the most popular drugs in the United States for treating Type 2 diabetes since 2007. It has only been on the market since 1999. The drug recently came under fire for causing an increased risk of congestive heart failure and its link to bladder cancer. The drug’s maker, Takeda, paid $2.37 billion to settle thousands of lawsuits by people who claimed Actos caused their bladder cancer.
AVANDIA (ROSIGLITAZONE):
This drug comes from the same controversial class of drugs as Actos, and works in a similar way. Studies link it to an increased risk of heart failure. A number of countries in Europe stopped selling the drug and banned it. Although not banned in the United States, it can only be prescribed by a small group of doctors.
TDS side effects may include:
- Bone fractures
- Macular edema
- Liver failure
- Heart failure
- Sinus infection
- Sore throat
- Fatigue
- Muscle pain
- Headache
- Skin rashes
- Hypoglycemia
SULFONYLUREAS AND NON-SULFONYLUREA SECRETAGOGUES
These drugs stimulate the pancreas to produce more insulin. There are several well-known Type 2 diabetes drugs that use sulfonylureas as their base. These include Glucotrol (glipizide), Diabeta (glyburide) and several others. The FDA approved the first of these drugs in the 1980s.
These work to decrease blood glucose levels by stimulating insulin release by the beta cells in the pancreas. Pancreatic beta cells are the cells primarily responsible for releasing insulin.
Side effects of sulfonylureas include:
- Nausea
- Dizziness
- Rash
- Diarrhea
- Weight Gain
DRUGS THAT SLOW DIGESTION OF CARBOHYDRATES
One of the issues with Type 2 diabetes is glucose entering the bloodstream faster than the body can process it. Slowing the digestive process of starches and sugars slows down the rate that glucose enters the bloodstream.
ALPHA-GLUCOSIDASE INHIBITORS AND AMYLIN ANALOGUES:
These drugs slow the digestion of sugar. Because these medications affect the digestive system, side effects of nausea and flatulence are common. Alpha-glucosidase inhibitors are the least effective medications for lowering blood sugar and are rarely used in the United States. Precose (acarbose) and Glyset (miglitol) belong to this class. Amylin analogues also have a modest effect on blood sugar, and are injected with a dosing pen. The only product available is called pramlintide.
DIPEPTIDYL PEPTIDASE-4 INHIBITORS (DPP-4):
These drugs keep the hormone incretin from being broken down, stimulating insulin production and slowing digestion. Popular brand names are Januvia, Onglyza and Tradjenta. Generic names are sitagliptin, saxagliptin and linagliptin. Side effects include: joint pain, pancreatitis, sore throat, swelling of hands or feet, nausea, hypoglycemia and diarrhea.
TAKING INSULIN
Everyone with Type 1 diabetes must take insulin every day. However, patients diagnosed with Type 2 diabetes sometimes need to take insulin as well, when oral medications taken along with diet and exercise, are no longer enough to control the disease on their own. Some reasons why people with Type 2 may need to start taking insulin, even if just temporarily, often involve other health conditions, injury, medication use or any other physiological change that can cause an individual’s body to become unable to produce enough insulin.
These reasons might include:
- Pregnancy
- Surgery
- Broken bones
- Cancer
- Steroidal medicine-use (such as Prednisone)
- Aging
- Weight gain
- Chronic (long-term, ongoing) emotional or physical stress
Insulin is injected under the skin (called a subcutaneous injection) using a syringe, insulin pen or insulin pump. The abdomen is the preferred injection site due to a more consistent absorption of insulin occurring in this region. However, the location for injections should be rotated regularly to avoid a condition called lipodystrophy, or erosion of the fat beneath the skin. Other popular injection sites include the thigh and the arm.
Insulin is not available to be taken in an oral form because stomach acid destroys the hormone. However, there is an inhaled version of the drug sold under the brand name Afrezza. This is a powder that is breathed in just before a meal (rapid-acting).
Doses of insulin vary by patient. How much insulin a patient requires daily depends on several factors, including:
- Weight
- Eating habits
- Exercise levels
- Other illnesses
- Level of insulin resistance (in Type 2 patients)
In patients with Type 2 diabetes, insulin may be stopped if temporary situations necessitating its use are resolved, or sometimes with weight loss, exercise or other lifestyle changes. Patients with Type 1 diabetes will never be able to stop taking insulin, although doses may be adjusted.
TYPES OF INSULIN AND SIDE EFFECTS
There are four different types of insulin that work differently for patients with diabetes — rapid-acting, short-acting, intermediate-acting and long-acting. Rapid-acting and short-acting insulins are often used in combination with longer-acting insulins. Both rapid- and short-acting insulins are taken shortly before meals (usually about 30 minutes prior) to cover the rise in blood glucose levels that results from eating.
Intermediate- and long-acting insulins cover any elevations in blood glucose levels after the shorter acting insulins stop working. Intermediate-acting insulin is usually taken twice a day, while long-acting insulin is taken once or twice a day.
The following chart breaks down the different types of insulin and how they work.
|
TYPE OF INSULIN
|
BRAND NAME
|
ONSET OF INSULIN’S EFFECTS
|
DURATION OF DOSE
|
|
Rapid-acting
|
Humalog Novolog Apidra
|
10 to 30 minutes (usually taken just before eating)
|
3 to 5 hours
|
|
Short-acting
|
Regular (R)
|
30 minutes to 1 hour (usually taken 30 minutes prior to a meal)
|
Up to 12 hours
|
|
Intermediate-acting
|
NPH (N)
|
1.5 to 4 hours
|
Up to 24 hours (but usually taken twice a day)
|
|
Long-acting
|
Lantus Levemir
|
About 45 minutes to 4 hours
|
Up to 24 hours
|
Insulin is generally considered safe to take. It is even the preferred drug, over oral drugs, to control blood glucose levels during pregnancy and when breastfeeding. However, insulin is not without side effects. Hypoglycemia (low blood sugar) is the most common side effect experienced in patients taking insulin.
Other Insulin Side Effects Might Include:
- Blurred vision (usually temporary after prolonged high blood sugar levels are returned to normal)
- Headache
- Skin reactions, including redness, swelling, itching or rash at the injection site
- Worsening of diabetic retinopathy (disease of the retina, or the nerve layer that lines the back of the eye)
- Changes in body fat distribution (lipodystrophy)
- Allergic reactions
- Sodium retention
- Swelling (edema)
- Weight gain
- Low potassium blood levels
- Throat pain or irritation, cough (associated with inhaled insulin)
Diet/Exercise
Healthy eating helps keep blood sugar down and is a critical part of managing both Type 1 and Type 2 diabetes, according to the National Institutes of Health. In fact, healthy eating is a part of a diabetic patient’s treatment plan, along with insulin for primarily Type 1 patients or another prescribed medication for patients with Type 2. Type 1 patients are also required to count carbohydrates and frequently monitor their blood sugar levels. Type 2 patients should be mindful of their blood sugar levels before and after eating as well.
The NIH recommends talking to a registered dietitian or nutritionist to develop an eating plan that works around each individual’s lifestyle, weight, medicines and other health problems. The National Institute of Diabetes and Digestive and Kidney Diseases has tips for healthy eating.
These include:
- Eating a lower sodium diet
- Eating smaller portions spread out over the day
- Keeping track of when and how many carbohydrates you eat
- Eating less fat
- Limiting alcohol consumption
- Eating a variety of vegetables, fruits and whole grains
Exercise is also beneficial for controlling blood glucose. Both Type 1 and Type 2 patients can benefit from exercising regularly and maintaining a healthy weight. A personal trainer or a diabetes expert can help you set meaningful goals. An exercise plan does not have to be strenuous to impart benefits.
What is type 2 diabetes and describe the disorder’s link to diet and exercise?
In fact, new research in the journal Diabetologia shows that short 10-minute walks after meals can help lower blood sugar. Researchers at the University of Otago in New Zealand found these short walks after meals helped control blood glucose better than a single 30-minute walk by 12 percent.
FACT
Other 2016 research in Diabetologia by Dr. Bernard Duvivier of Maastricht University in the Netherlands found simply sitting less and by standing more and doing light walking may control blood sugar better than higher intensity exercise.
SPECIAL CONSIDERATIONS
Exercise can cause blood sugar levels to drop, especially in diabetic patients taking insulin. Patients with diabetes should regularly monitor their blood sugar levels before, during and after physical activity to make sure they don’t get too low.
Additionally, after administering insulin, strenuous activity can potentially speed up the body’s absorption of the hormone. Patients who plan to exercise following an insulin injection, should not inject themselves in an area that is most likely to be affected by the activity. For example, patients who plan to go running soon after the injection of insulin, should not inject the hormone into their thigh.
Bariatric Surgery
Bariatric surgery is growing in popularity as a treatment for Type 2 diabetes. There are a few methods of performing the surgery, but they all involve shrinking the size of the stomach or rerouting the path of food.
As with any surgery, there are risks, including:
- Poor nutrition
- Vomiting from eating too much
- Scarring that could lead to blockages
- Injury to the stomach and intestines
- Heartburn or ulcers
- Leaking from stomach incisions
The most familiar type of surgery is gastric bypass. It creates a small pouch at the top of the stomach about the size of a walnut. The surgeon then reconnects the small intestine to this new walnut-sized stomach.
One study published in 2011 in Diabetes Care showed the surgery is highly effective in very obese patients with Type 2 diabetes. A review of clinical literature showed diabetes death rates lowered by up to 90 percent after gastric-bypass surgery.
Overweight patients with poorly controlled Type 1 diabetes may make good candidates for surgery as well. Such operations may give Type 1 patients greater control over the disease — not a cure.
They may experience a possible reduction in daily insulin doses, according to a review of cases from the Cleveland Clinic in Ohio.
One study conducted at Cleveland Clinic showed that 9 out of 10 morbidly obese patients with Type 1 who underwent a laparoscopic procedure, such as a gastric bypass, lost more than 60 percent of their body weight in more than three years’ time. These patients also saw improvements in all cardiovascular risk factors, such as hypertension (high blood pressure) and triglyceride levels (the most common type of fat found in the blood).
Other Pages Related to Diabetes
Farxiga Side Effects
Farxiga side effects include bladder cancer, ketoacidosis, kidney injury and serious urinary tract infections. Some patients have died.
Farxiga Side Effects
SGLT2 inhibitors like Invokana and Farxiga are used to treat Type 2 diabetes. However, several studies have linked these drugs to serious conditions.
SGLT2 Inhibitors
SGLT2 inhibitors like Invokana and Farxiga, are popular Type 2 diabetes drugs, but FDA released several safety communications about side effects.
Diabetes Complications
Diabetes is a serious condition that can result in serious complications if not managed properly. All diabetes complications are the result of poorly controlled blood glucose levels. When blood glucose levels are controlled in both patients with Type 1 and Type 2 diabetes, short- and long-term complications can be prevented or postponed.
One of the most common short-term diabetes complications, especially in patients with Type 1 diabetes, is hypoglycaemia, or low blood sugar. This is due to taking too much insulin or not properly planning insulin intake around meals and/or exercise. Certain medications, such as aspirin, and alcohol can sometimes cause hypoglycemia in patients with diabetes, as well.
While many people with Type 2 diabetes might not immediately notice symptoms of the disease, it can still cause serious complications if left untreated. Even after diabetes complications develop, maintaining control over one’s blood sugar levels can assist in managing symptoms and preventing additional problems.
Diabetic Ketoacidosis (DKA)
While diabetic ketoacidosis (DKA) is a side effect of some Type 2 diabetes medications such as Invokana, people with both Type 1 and Type 2 diabetes are at increased risk even without taking the medication. Lack of insulin production can lead to DKA. This occurs when the body cannot use glucose for fuel and burns fat instead. The by-products of breaking down fat for fuel are called ketones. When ketones build up in the body, they become toxic.
This condition is rare in people with Type 2 diabetes, though, and usually affects people with Type 1 diabetes whose bodies do not produce insulin at all.
Sometimes, people do not realize they have diabetes until they develop DKA.
Risk of Pancreatitis and Pancreatic Cancer
People with both types of diabetes are at increased risk for pancreatitis (swelling of the pancreas) and pancreatic cancer.
Acute pancreatitis may happen suddenly and symptoms include pain in the abdomen, nausea, fever and rapid heartbeat. Chronic pancreatitis develops over time and symptoms include oily stools, diarrhoea, weight loss and vomiting. One study published in Diabetes Care found that people with Type 2 diabetes were almost twice as likely to have acute pancreatitis as people without Type 2. But researchers found insulin slightly decreased this risk. Pancreatitis can lead to pancreatic cancer.
Diabetes can be a risk factor or a symptom of pancreatic cancer. Typically, this type of cancer is more prevalent in people who have had diabetes for more than five years, according to the Pancreatic Cancer Action Network. Researchers found that health conditions connected to Type 2 diabetes such as insulin resistance, inflammation and high blood sugar all contribute to development of pancreatic cancer. But people with pancreatic cancer may also develop diabetes as a symptom of the cancer.
Some Type 2 diabetes medications may also increase the risk of pancreatitis and possibly pancreatic cancer, including DPP-4 inhibitors such as Januvia, Janumet and Victoza.
Increased Mortality
Diabetes also increases mortality. Diabetes was mentioned as a cause of death on 234,051 death certificates in 2010, according to American Diabetes Association statistics. The ADA also says diabetes may be underreported as the cause of death.
Other Diabetes Complications Include:
- Eye complications
- High blood pressure
- Skin problems
- Nerve damage (neuropathy)
- Heart disease
- Amputation of limbs
- Heart stroke
- Kidney disease
Pregnancy and Diabetes
Uncontrolled Type 1 or Type 2 diabetes is especially dangerous during pregnancy. Not only does it affect the mother, but it can also endanger the baby. A foetus’ organs are formed within the first two months of pregnancy, often before a woman knows she is pregnant. Blood sugar that is too high (or too low) can affect the organs as they are developing leading to serious birth defects. Therefore, women planning to get pregnant should make sure they have their blood sugar under control before and during pregnancy.
High blood sugar before and during pregnancy can:
- Increase the risk of birth defects, such as those of the brain, spine and heart
- Increase the risk of miscarriage or stillbirth
- Increase the risk of having a large baby, which also increases a mother’s risk of having to deliver by caesarean section (C-section)
- Worsen long-term complications of diabetes, including, kidney disease, heart disease and eye problems
- Increase problems for the baby such as premature birth, nerve damage, breathing problems or low blood sugar after birth
Preeclampsia
Women with diabetes are at a higher risk of preeclampsia during and after pregnancy. Preclampsia is one of the leading causes of child-bearing related death. Most deaths happen in the days or months after the mother gives birth. Preeclampsia can be treated. And most deaths are preventable if a woman receives treatment.
Symptoms of preeclampsia during and after pregnancy include:
- Abdominal pain
- Anxiety
- Decreased urination
- Excess protein in the mother’s urine
- Headache
- High blood pressure (140/90 or higher)
- Hyperreflexia (over-reactive reflexes)
- Lower back pain
- Nausea or vomiting
- Severe Headaches
- Shortness of breath
- Shoulder pain
- Stomach problems or pain
- Sudden weight gain
- Swelling
- Swelling
- Vision changes
Health care providers should continue to monitor women for signs and symptoms of preeclampsia after they give birth. Postpartum preeclampsia symptoms may mimic those of other conditions new mothers experience. These can include headaches, stomach problems and swelling.
Gestational Diabetes
About seven out of every 100 pregnant women in the U.S. suffers from gestational diabetes. Gestational diabetes is diabetes that happens for the first time during pregnancy, usually around the 24th week, according to the American Diabetes Association (ADA). Gestational diabetes is not the same condition as a person already diagnosed with Type 1 or Type 2 diabetes who then gets pregnant.
A diagnosis of gestational diabetes does not mean that a woman had diabetes prior to conceiving. Additionally, gestational diabetes generally goes away after pregnancy. However, it can increase a woman’s chances of developing Type 2 diabetes later in life. The infant may also be at an increased risk for obesity and Type 2 diabetes.
Pregnant women are typically tested for diabetes during the second trimester of the pregnancy as a part of routine prenatal care. Gestational diabetes is caused by hormones from the placenta that block the body’s normal use of insulin and prevent the body from regulating the increased blood sugar levels that are usually associated with pregnancy.
Symptoms of gestational diabetes are similar to those of Type 1 or Type 2 diabetes, including:
- Unusual thirst
- Frequent urination in large amounts versus the frequent but normally light amounts seen in early pregnancy
- Fatigue, which can be hard to detect due to the fatigue caused by pregnancy itself
- Sugar in the urine, which can be found via a urine sample during a routine prenatal visit
A test for gestational diabetes may be done earlier if a woman is considered to be at higher risk for developing the disease. Risk factors include being overweight, older, having a history of gestational diabetes from previous pregnancies and receiving a pre-diabetes diagnosis before pregnancy.
Staying active and maintaining a normal (or healthy weight), as well as eating a healthy, well-balanced diet, are ways in which women can help prevent the development of gestational diabetes.
Here are some tips for a healthy pregnancy:
- Quit smoking
- Check blood glucose levels often
- Have a diabetes and pregnancy care team in place
- Check ketone levels through urine or blood
- Keep regular appointments with your doctor
- Eat a proper diet
- Avoid alcoholic beverages
- Daily physical activity
- Check medications to see if they may affect the baby
Type 1 Diabetes Research
The American Diabetes Association (ADA) is focused on improving the lives of all people affected by diabetes. While Type 2 makes up the majority of those individuals, Type 1 is a priority of the nonprofit health organization as well. In 2016, 37 percent of the nonprofit’s total research budget was apportioned to projects relevant to Type 1.
Smart Insulin Patch
One recent project, started in early 2015, that would benefit people with Type 1 as well as those with advanced Type 2 requiring insulin, is the smart insulin patch. ADA Pathway to Stop Diabetes scientist Zhen Gu, a professor in the Joint University of North Carolina/North Carolina State University Department of Biomedical Engineering, published a paper in the biomedical journal, Proceedings of the National Academy of Sciences, describing the development of the new patch that could replace painful and burdensome injections.
The smart insulin patch, made of thin silicon, is about the size of a penny. It includes more than 100 microneedles, each one approximately the size of an eyelash. The microneedles house live beta cells that can sense when blood glucose levels are high and send a rapid release of insulin into the patient’s bloodstream. The live beta cells (cells responsible for making insulin) are said to reduce the risk of complications and last longer than the synthetic insulin that was previously preloaded in the patch.
The final prototype is expected to include glucagon (the hormone responsible for counteracting insulin) into the device as well. This will make the smart insulin patch effective in correcting both high blood glucose levels as well as low blood glucose levels (hypoglycaemia), a dangerous potential side effect of taking insulin.
Scientists have tested the smart insulin patch technology in mouse models, where it was discovered that the device was able to effectively lower blood glucose levels for up to nine hours. The positive result paves the way for continuing research in live animals and eventually clinical trials for humans.
Immunotherapy Clinical Study
British researchers published results from a small clinical trial showing immunotherapy treatment is safe for people with Type 1 diabetes. Science Translational Medicine published the findings from the study in August 2017, reporting that the immune system therapy showed promise in maintaining insulin production in people who were newly diagnosed with the disease.
The immunotherapy treatment is comparable to an allergy shot in how it works in that it is supposed to stop the immune system from attacking the body, specifically the beta cells found in the pancreas responsible for making insulin.
Scientists determined that people who develop Type 1 diabetes likely do not produce enough of the right kind of T-regs, immune cells that can aid in the suppression of immune attacks, or the T-regs aren’t working as they should. So, researchers developed the treatment called peptide immunotherapy using disease-related autoantigens, substances that cause autoimmune attacks, in an attempt to “re-educate” the immune system and induce more, or more effective, T-regs.
ABOUT THE STUDY
The study involved 27 patients with Type 1 diabetes who had been diagnosed with the disease within the past 100 days. The participants were divided into three groups, including a group given placebos (dummy pill). Those taking the placebos increased their insulin-use by 50 percent over a 12-month period.
Although, all of the participants still required daily insulin, researchers asserted that the need for less insulin over time can lessen complications and improve patients’ overall quality of life.
Additional trials are needed to determine how often the immunotherapy treatments would need to be administered and what benefit, if any, it would have in people who have had Type 1 diabetes for a longer amount of time, whose beta cells are likely more severely damaged or altogether gone. Detectable C-peptide (a substance created along with insulin) levels in patients might also make a difference in this or future treatments.
One of the study’s authors and professor of clinical immunology at King’s College in London, England, Dr. Mark Peakman, said the next step “will be bigger trials to test whether the therapy can halt beta cell damage.”
Beta Cells Transplantation
Researchers with the ADA are working on ways to enhance the survival of beta cells for eventual successful transplantations for patients with Type 1 diabetes. The goal of such treatment is to replace insulin injections and provide better control of blood glucose levels.
Currently, there is a shortage of sufficient donor cells, further complicated by the fact that it takes several donors to transplant one recipient. The survival rate of these stem cells contained on islets, or small isolated masses of one type of tissue, is also very low, with 80 percent of transplanted islets dying from exhaustion. However, there is evidence to suggest that these beta cells can be trained to survive exposure to oxygen and nutrient shortages experienced before and after transplantation.
The ADA contends that stem cell technology resulting in an unlimited source of beta cells may very well be a reality in the next several years. Research to determine how best to use these new cells, how they live and function after transplantation, and how to control the body’s immune responses to the transplanted tissue, to avoid rejection or subsequent cell and tissue death, will be essential in the potential realization of an eventual cure for diabetes.
Type 2 Diabetes Research
Type 2 diabetes research focuses on four main areas: education, new technology and medications, prevention of the disease and prevention of complications. In addition to government funding of research, many drug companies also conduct their own studies to find new medications for the disease. The American Diabetes Association (ADA) also funds studies.
Some of the questions researchers may ask include:
- Who is at risk for Type 2 and what are the first signs of the disease?
- Can Type 2 diabetes be reversed?
- What are the physical differences between people with and without the disease?
- What new technologies make living with diabetes easier for patients?
- Why does Type 2 run in families?
- How can complications develop and how can they be prevented?
Some of the most recent findings include:
Dr. Marilyn Corneli, a nutritionist and assistant professor at Northwestern University Feinberg School of Medicine, found people who drink coffee have a lower risk of Type 2 diabetes, and she is doing more research to find out why.
Dr. Rebecca Hasson, an exercise physiologist at University of Michigan, found a link between environmental stress and Type 2 diabetes. Research suggests that when under stress, the body produces a hormone called cortisol. Cortisol contributes to insulin resistance.
Dr. Laura D. Baker found aerobic exercise improves brain function in people with prediabetes. Type 2 diabetes and prediabetes are the second biggest risk factors for Alzheimer’s. Diabetes increases the risk by 65 percent. Even small amounts of exercise improve cognition.
Please seek the advice of a medical professional before making health care decisions.

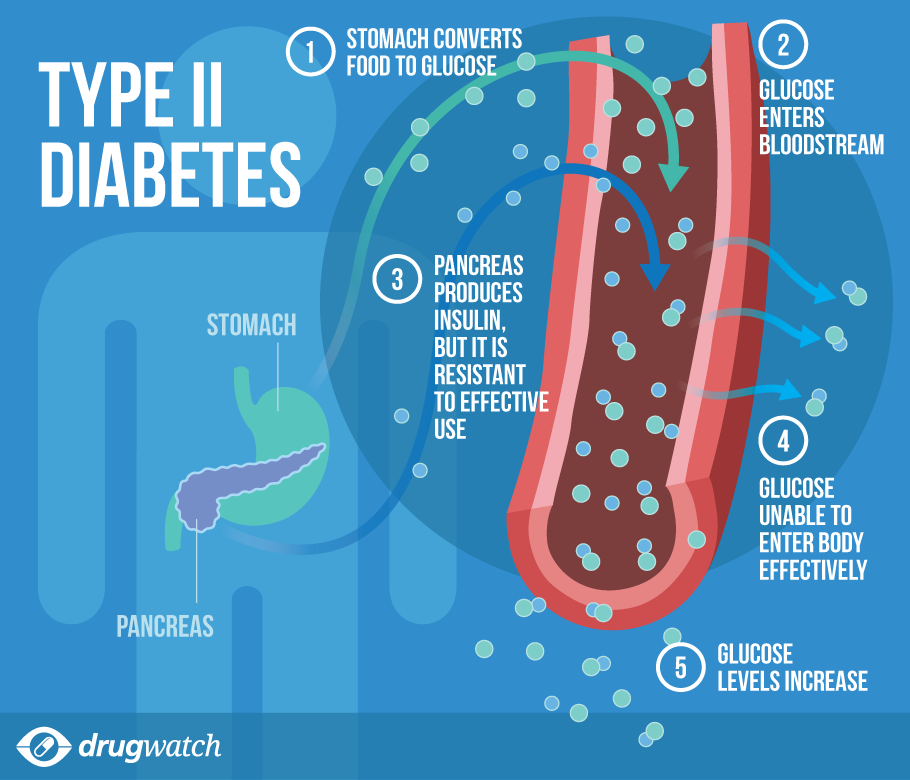{kind=link}